Xiao-fang Zhou1 ![]() ,
Zeng Wang1,
Yan-min Shen2,
Yi-tao Chen3,
Xiao-xian Xu4,
Ling-ya Chen1,
Lu-chao Chen3
,
Zeng Wang1,
Yan-min Shen2,
Yi-tao Chen3,
Xiao-xian Xu4,
Ling-ya Chen1,
Lu-chao Chen3
For correspondence:- Xiao-fang Zhou Email: zhouxiaofang133494@163.com Tel:+8657188122435
Received: 14 October 2015 Accepted: 7 August 2016 Published: 30 September 2016
Citation: Zhou X, Wang Z, Shen Y, Chen Y, Xu X, Chen L, et al. Effect of Prunella vulgaris L extract on hyperprolactinemia in vitro and in vivo. Trop J Pharm Res 2016; 15(9):1935-1939 doi: 10.4314/tjpr.v15i9.18
© 2016 The authors.
This is an Open Access article that uses a funding model which does not charge readers or their institutions for access and distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0) and the Budapest Open Access Initiative (http://www.budapestopenaccessinitiative.org/read), which permit unrestricted use, distribution, and reproduction in any medium, provided the original work is properly credited..
Purpose: To investigate the anti-hyperprolactinemic activity of Prunella vulgaris L. extract (PVE) in vivo and in vitro.
Methods: Rats were given intraperitoneal (i. p.) metoclopramide (MCP, 150 mg/kg daily) for 10 days to prepare hyperprolactinemia (hyperPRL) model. Bromocriptine was used as positive control drug. High (5.6 g/kg), medium (2.8 g/kg) and low (1.4 g/kg) doses of PVE were administered to hyperPRL rats. The effect of PVE on serum prolactin (PRL), estradiol (E2), progesterone (PGN), follicle stimulating hormone (FSH) and luteinizing hormone (LH) levels were investigated in the rats. MMQ cells derived from rat pituitary adenoma cells and GH3 cells from rat pituitary lactotropictumoral cells were used for in vitro experiments. The effect of PVE on PRL secretion were studied in MMQ cells and GH3 cells respectively.
Results: Compared with the control group (446.21 ± 32.43 pg/mL), high (219.23 ± 10.62 pg/mL) and medium (245.47 ± 13.52 pg/mL) reduced PRL level of hyperPRL rats significantly (p 0.05). In MMQ cells, treatment with 5 mg/mL PVE or 10 mg/mL PVE) significantly suppressed PRL secretion and synthesis at 24h compared with controls (p < 0.01). Consistent with D2- action, PVE did not affect PRL in rat pituitary lactotropic tumor-derived GH3 cells that lack the D2 receptor ex
Conclusion: PVE showed anti-hyperPRL activity and can potentially be used for the treatment of hyperprolactinemi, but further studies are required to ascertain this.
Introduction
Hyperprolactinemia is the most common disorder of the hypothalamic-pituitary axis. Patients typically present with hypogonadism, infertility or, in the case of macroadenomas, symptoms related to mass effect (headache and visual field defects) [1]. The incidence rate of hyperPRL was 0.4 % in the normal adult population and 9 -17 % in women with menstrual problems [2,3]. The two most commonly prescribed drugs in the treatment of hyperprolactinemia are bromo-criptine and cabergoline. Both medications are dopamine receptor agonists and share many characteristics and adverse effects, such as headache, nausea and vomiting, among others, though frequency and severity of adverse effects appears to be less in cabergoline compared to bromocriptine. It has been reported that 12 % patients cannot endure bromocriptine, which is one of the most widely used synthetic drugs in clinics [4].
Traditional Chinese medicine are often used for the treatment of hyperPRL [5]. Prunella vulgaris L. is a famous herb in China and widely used for treating hyperprolactinemia [6,7]. Most conventional anti-hyperPRL agents reduce PRL secretion through D2 receptor in the hypothalamic-neuroendocrine dopaminergic system [8]. Other sex steroids are also involved in the pathophysiology of hyperPRL [9]. In this study, the effects of PVE on serum hormone levels in hyperPRL rats and PRL secretion in cell-culture systems were investigated. MMQ cell derived from rat pituitary adenoma cells and GH3 cell derived from rat pituitary lactotropictumoral cells were used.
Methods
Preparation of PVE
The dried herbs of Prunella vulgaris L. were mixed, and decocted with 1000 ml of water in a decocting pot twice, 45 min for each. The filtrate was mixed and concentrated into 200 ml liquor of PVE. It was then filtered through a 0.2 μm filter, and used for both in vitro and in vivo experiments.
In vivo animal studies
Female SD rats weighing 150 - 180 g were obtained from Zhejiang Center for Disease Control and Prevention, Hangzhou, Zhejiang. The animals had free access to feed and water, and were allowed to acclimatize for at least one week before use. All experiments were approved by the Animal Care and Use Committee of Zhejiang Cancer Hospital (approval ref no. 20120622) and carried out in compliance with Directive 2010/63/EU on the handling of animals used for scientific purposes [10].
Rats were given intraperitoneal (i.p.) metoclopramide (MCP, 160 mg/kg body weight daily) for 10 days to prepare the model of hyperPRL [11]. 60 rats were randomly divided into six groups of ten rats: control, model group, bromocriptine-treated group, high-dose PVE-treated (5.6 g/kg body weight) group, middle-dose PVE-treated (2.8 g/kg body weight) group and low-dose PVE-treated (1.4 g/kg body weight) group. Each dose was dissolved in 2 mL water, and administered by gavage. The dosage was calculated from the human clinical dosage of PVE based on body surface area. Control and untreated model rats received 2 mL of saline. All the mice received treatment for 30 days. After the last treatment, serum PRL, E2, PGN, FSH and LH levels of the rats were measured by ELISA.
Cell lines and cell culture studies
MMQ cell and GH3 cell were used for in vivo experiments. MMQ cell was derived from rat pituitary adenoma cells, and GH3 cell was derived from rat pituitary lactotropic tumoral cells. Dose-dependent and time-course responses of PRL secretion and synthesis to PVE treatment were evaluated in MMQ cell line.
MMQ cells were treated with PVE at concentrations of 1 - 10 mg/mL for 12 – 48 h. At different incubation time points, the culture medium was collected for measuring PRL secretion. Cells were collected for determining cellular PRL expression. The optimal concentrations and treatment duration were then determined for subsequent experiments. GH3 were treated with PVE at effective concentrations that had been determined in MMQ cells for 24 h. The GH3 cells and medium were collected for the measurement of PRL secretion and expression respectively.
Hormone assay
Serum PRL, E2, PGN, FSH and LH concentrations of rat and PRL concentrations in the culture medium collected from MMQ and GH3 cells were measured using ELISA kits (Nanjing Jiancheng Biological Engineering Co, Ltd).
Statistical analysis
One- or two-way analysis of variance (ANOVA) was used to detect statistical significance, followed by post-hoc multiple comparisons (Student-Newman-Keuls method). Data are expressed as mean ± SEM. Statistical significance was defined as p < 0.05.
Results
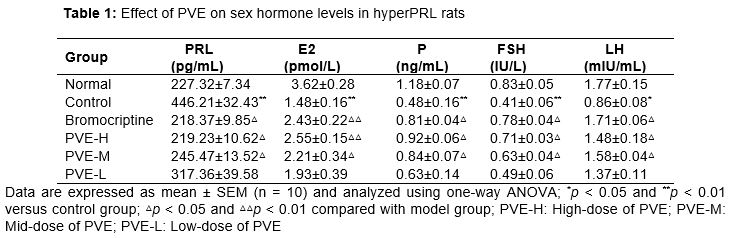
Effect of PVE on sex hormone levels in hyperPRL rats
Compared with the control group, serum PRL level of hyperPRL model rats increased significantly (p < 0.01). Serum E2, PGN, FSH and LH levels of hyperPRL model rats decreased significantly (p < 0.01) after injecting metoclopramide in abdominal cavity. Compared with the control group, the increased PRL level was significantly attenuated by treatment with 0.5 mg/kg bromocriptine and 2.8 or 5.6 g/kg PVE after 30 days (p < 0.01). And rat serum E2 level increased (p < 0.01), and serum PGN, FSH and LH levels increased (p < 0.05) significantly in bromocriptine- treated group. Compared with the control group, rat serum E2 level increased (p < 0.01), and serum P, FSH and LH levels increased (p < 0.05) significantly in high-dose of PVE group ().
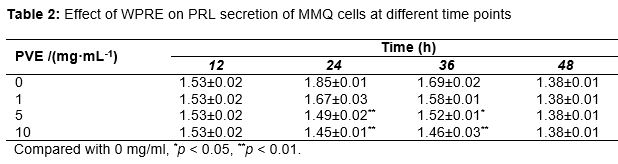
Effect of PVE on hyperactive PRL in MMQ and GH3 cells
Two-way ANOVA analysis revealed a significant interaction between time course and treatment dose (F = 2.227, p = 0.042). Post-hoc multiple comparison further revealed that 1 and 10 mg/mL PVE treatment for 24 and 36 h, but not 12 and 48 h, produced significant suppression of PRL concentrations in the MMQ culture medium compared with controls (0 mg/mL) (p < 0.005) (). 24 h was then used in the latter experiment. PVE treatment for 24 h also yielded a significant suppression of MMQ cellular PRL expression in a dose-dependent manner (F = 23.557, p < 0.001). Compared to control, the significant suppression was observed in the higher two concentrations (5 and 10 mg/mL) (p < 0.003) (Tab. 2). The same concentrations did not produce significant effects on the medium concentration (F = 2.248, p = 0.136) and the cellular expression (F = 0.253, p = 0.812) in GH3 cells ().
Discussion
Hyperprolactinemia is a common endocrinological disorder that may be caused by several physiological and pathological conditions. Several drugs may determine a significant increase in prolactin serum concentration that is frequently associated with symptoms. In this study, we used the hyperPRL model of rats and two cell models to investigate the effect and action mechanism of PVE. MMQ cells, which express D2 receptor, are an excellent model of hyperPRL derived from rat pituitary adenoma cells responsive to dopamine [12]. Dose-dependent and time-course responses of PRL secretion and synthesis to PVE treatment were evaluated in this cell line. GH3 cells were derived from rat pituitary lactotropictumoral cells that lack D2 receptor expression [13,14], which were used to determine if deficiency of D2 receptor saltered the suppression of PVE on hyperactive PRL.
Consistent with D2-action, PVE did not affect PRL in rat pituitary lactotropic tumor-derived GH3 cells that lack the D2 receptor expression. Our study result showed that D2 receptor is necessary for anti-hyperPRL activity of PVE. It suggest that D2 receptor played important roles in anti-hyperPRL activity of PVE.
Dopamine receptors belong to the family of seven transmembrane domain G-protein coupled receptors (GPCR) [15-17].Dopamine receptors D1 and D2 are classified into two subtypes based on their differential effect on adenylylcyclase.
Classically, the functions of dopamine receptors have been associated with the regulation of adenylate cyclase-protein kinase A through G-protein-mediated signaling. Two classes of GPCR mediate dopamine functions, D1-like receptor sub-types (D1 and D5) couple mostly to Gas and stimulate the production of the second messenger cyclic adenosine monophosphate (cAMP) and the activity of protein kinase A (PKA). By contrast, D2-like subfamily (D2, D3 and D4) couple to Gai/o and regulate the production of cAMP thus resulting in a diminution of PKA activity [18-20]. The physiological and pathological roles of DR2 have been recognized in some organs such as brain and kidney [21,22]. In the adenohypophysis, the predominant dopamine receptor is D2 receptor [23]. Transfection of the dopamine D2 receptor into a pituitary cell line results in a decrease in intracellular cAMP and inhibits prolactin secretion when dopamine is added to the cell culture [24]. Most conventional anti-hyperPRL agents reduce PRL secretion through D2 receptor in the hypothalamic neuroendocrine dopaminergic system. This study revealed that PVE showed anti-hyperPRL activity via dopamine D2 receptor.
Conclusion
The findings of the study indicate that Prunella vulgaris L. extract possesses anti-hyperprolactinemic activity in vivo and in vitro, and therefore, can potentially be developed for therapeutic management of hyperprolactinemia.
References
Archives


News Updates